


Opinion on the paper: Duration of mRNA vaccine protection against SARS-CoV-2 Omicron BA.1 and BA.2 subvariants in Qatar
A lesson in Cognitive Bias

The last video from Drbeen Medical Lectures titled Unvaccinated vs Vaccinated PROTECTION from COVID - Qatari Cohort | New Studies brought to my attention this study from Qatar,
Duration of mRNA vaccine protection against SARS-CoV-2 Omicron BA.1 and BA.2 subvariants in Qatar
which again, shows how effectiveness against symptomatic infection declines over time, considerably I would say, and effectiveness against any severe, critical, or fatal COVID-19 is strong and durable.
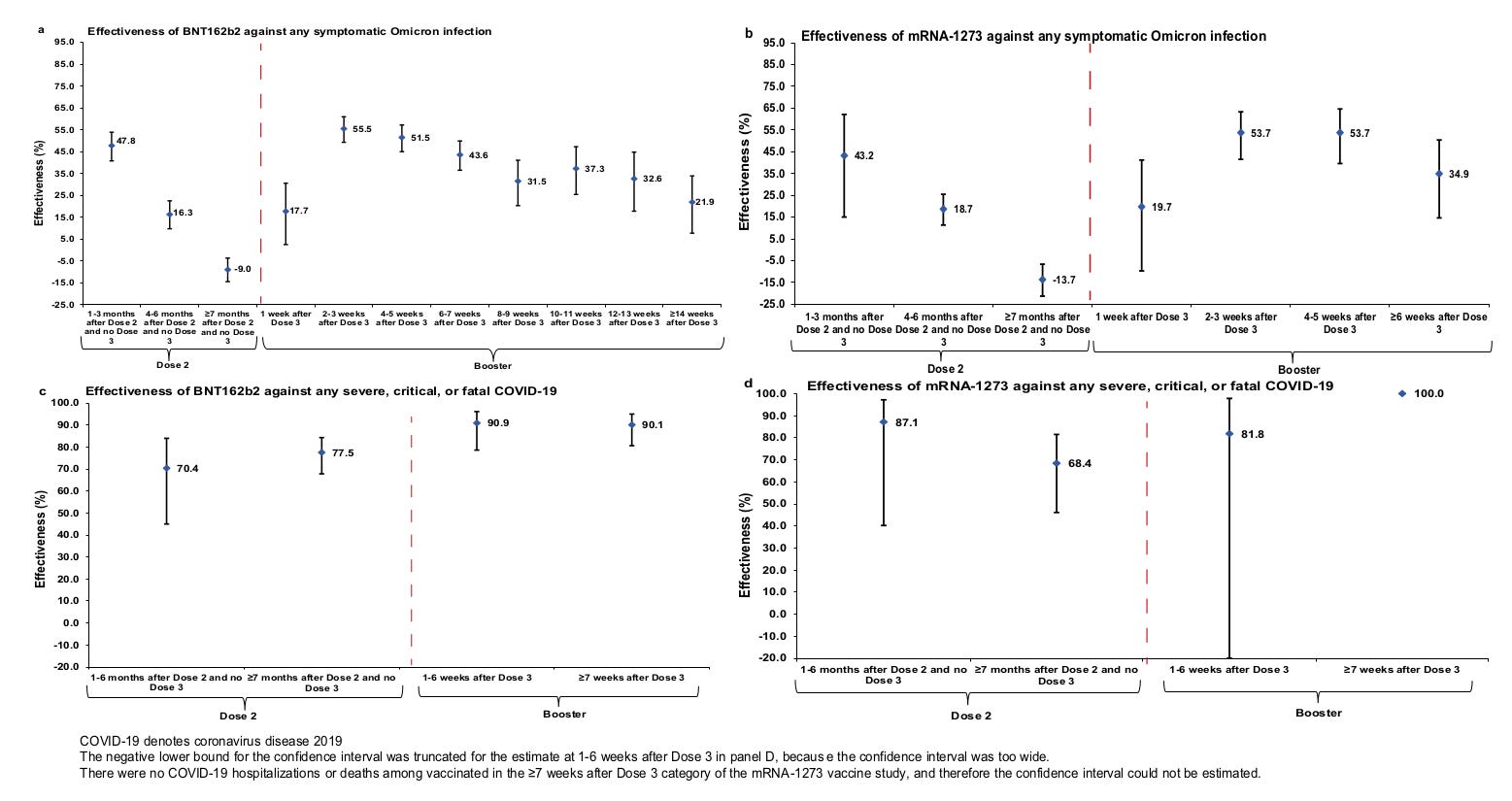
This was estimated using the test-negative, case–control study design.
Following their references (The test-negative design for estimating influenza vaccine effectiveness),
“Under the test-negative design for influenza VE, study subjects are all persons who seek care for an acute respiratory illness (ARI). All subjects are tested for influenza infection. Influenza VE is estimated from the ratio of the odds of vaccination among subjects testing positive for influenza to the odds of vaccination among subjects testing negative.”
and their indications,
“Cases (persons infected with BA.1, BA.2, or any-Omicron-sub-variant) and controls (uninfected persons) were exact-matched by sex, 10-year-age group, nationality, and calendar week of polymerase chain reaction (PCR) test to control for established differences in the risk of exposure to SARS-CoV-2 infection in Qatar.”
seems to be that controls were individuals seeking care for an acute respiratory illness who tested negative for SARS-CoV-2 Omicron infection.
THE PROBLEM:
Having established that, let’s take a look to Table 5
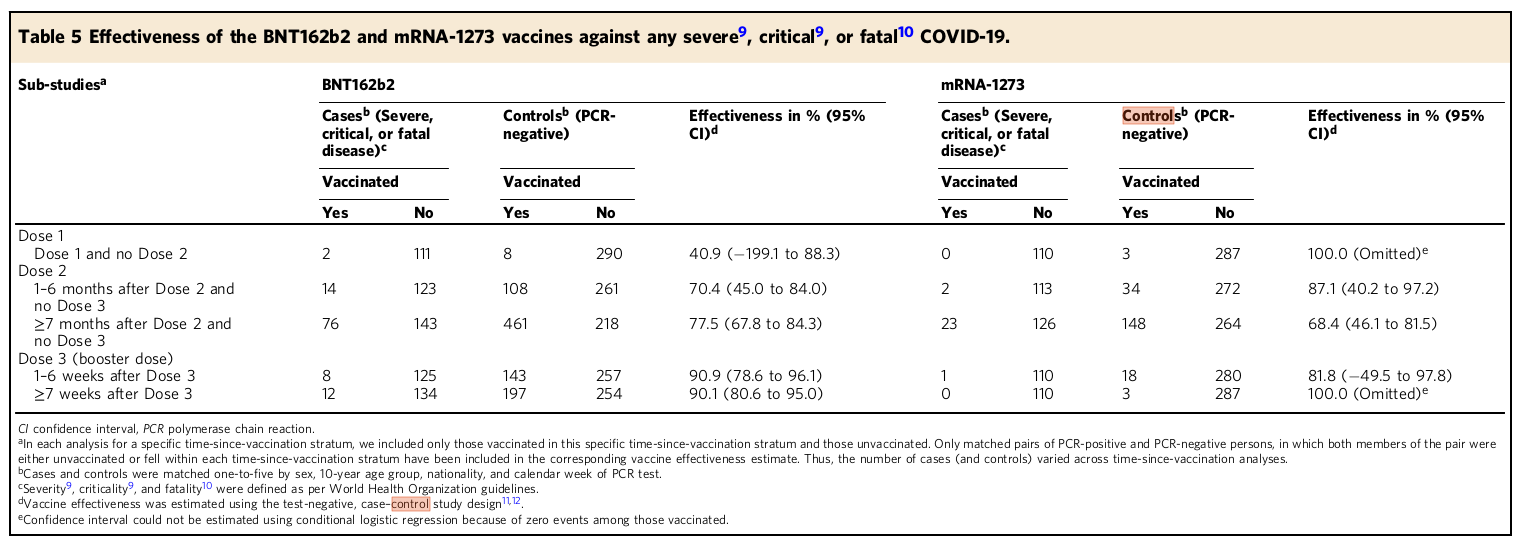
and let’s pay attention to the controls, which in principle do not have a SARS-CoV-2 infection.
In Dose 1 for instance, the number of cases is so low in the vaccinated cohort compared to the unvaccinated that for BNT162b2 the confidence interval takes negative values. It cannot even be calculated for mRNA-1273 because you have to divide by 0 (for more on confidence intervals take a look to my previous substack - Pfizer Vaccine Efficacy & Confidence Interval).
On the one hand, the confidence interval indicates that you cannot established any validity to these numbers. On the other hand, the values in the control group indicate a clear bias in the behavior and overall health of both populations (vaccinated vs unvaccinated) in Qatar. You would expect for a very similar number of non-COVID-19 events in the controls, while they are separated by two orders of magnitude in Dose 1.
BNT162b2: A difference of 8 events to 290 events between cohorts in the Controls?
mRNA-1273: A difference of 3 events to 287 events between cohorts in the Controls?
If we focus now in the controls for Dose 2 and Dose 3, we see something even more odd. Unvaccinated controls keep a consistent number of events during the whole period while vaccinated controls considerably increase the number of severe, critical, or fatal non-COVID-19 events during Dose 2.
BNT162b2 —> (Dose 1) 8 - (Dose 2) 108, 461 - (Dose 3) 143, 197
mRNA-1273 —> (Dose 1) 3 - (Dose 2) 34, 148 - (Dose 3) 18, 3
Almost as if they are becoming sicker and sicker for some reason.
If this was the case, only the healthiest between them would have taken the 3rd Dose. Hence, we can explain to some extend why the numbers for the vaccinated controls suddenly drop after Dose 3. In the case of Moderna, the numbers may be so low after Dose 3 due to higher promotion of the Pfizer boosters, new healthcare recommendations and guidelines not recommending Moderna for certain age groups…
CONCLUSION:
The authors’ claim
“vaccine protection against COVID-19 hospitalization and death is strong and durable after the second dose, and is most robust after a booster dose”
is not a valid statement.