

Epigenetic shifts and Microbiome genome integration after SARS-CoV-2 transfections?
Epigenetic shifts and Microbiome genome integration after SARS-CoV-2 transfections?

First of all I would like to refer the reader to the excellent articles wrote by Igor Chudov on this topic:
Pfizer's COVID Vaccine Causes VAIDS in Children, Study Proves
[NOTE: Just to be fair, I will add at the end my perspective on why I think the study does not prove that Pfizer’s transfections cause the so-called VAIDS]
Half of Vaccinated People Never Stop Producing Spike Protein, Study Found
My perspectives on the issue and my comment:
[Reference to my comment to Igor Chudov] [Update in relation to another study, my comment here]
I am reading the paper now. [Detection of recombinant Spike protein in the blood of individuals vaccinated against SARS-CoV-2: Possible molecular mechanisms] [Ref 0.1]
Just to be sure I did a BLAST search of the PP-Spike peptide LDPPEAEVQIDR and although some of the results say that is present in SARS-CoV-2 if you go to the papers they are all Chain A, spike glycoprotein studies in which they use recombinant spike with proline substitutes to test for antibody responses. Thus, it is safe to say that it is a marker of the vaccines.
With regards to their three main hypothesis, given the persistence, clear signal and ubiquitousness of their findings I am incline to believe that the most likely explanation is the assimilation of the genetic material by bacteria in the microbiome. Chromosomal integration or intra-nuclear localization would not happen so persistently in all subjects and it would not necessarily be active in the subset of cells that would be affected.
In any case, this is quite concerning and it also may explain the epigenetic shift that was found in the paper you shared yesterday in relation to the cytokine and toll-like receptor agonists response to heterologous pathogens. [BNT162b2 COVID-19 vaccination in children alters cytokine responses to heterologous pathogens and Toll-like receptor agonists] [Ref0.2].
Even though it is not easy to interpret the clinical significant of such shifts I did some searches on PubMed and the best review that I found was [A systems immunology approach to investigate cytokine responses to viruses and bacteria and their association with disease] [Ref1]
I will share some quotes from the paper here:
"Patterns of human immune responses to viruses and bacteria and how this impacts risk of infections or onset/exacerbation of chronic respiratory diseases are poorly understood."
"we measured peripheral blood mononuclear cell responses (28 cytokines) to respiratory viruses and bacteria, Toll-like receptor ligands and phytohemagglutinin, in 307 children. Cytokine responses were highly variable with > 1000-fold differences between children."
Their results agree with the ones obtained in this other paper [Inter-individual variability and genetic influences on cytokine responses to bacteria and fungi] [Ref2], where the cytokine profile and presentation clusters around, I quote from [Ref2], "a physiological response to specific pathogens, rather than around a particular immune pathway or cytokine". In [Ref1] we can see this clearly in the patterns presented for virus stimulation vs bacterial stimulation in Fig.1. (below)


It is important to notice that there is a distinct presentation for IL-17. In [Ref2] they state "One remarkable exception to the rule of pathogen-centric responses is represented by specific lymphocyte responses such as IL-17 production, which represents a separate strongly correlated cluster independent of the type of pathogen and may be an important aspect of IL-17 biology." In [Ref1] they found that "The other subgroup included IL-17, CCL2/MCP1 and CCL13/MCP4, among which IL-17 was induced very strongly by PHA, moderately by PGN and weakly by other stimuli."
I think this is key to understand the relevance of the paper at hand [Ref0.2] because IL-17 should have, it seems, as far as my research goes, a very weak response to virus stimuli. However, as we can see in [Ref0.2] (image below) the IL-17 response to SARS-CoV-2 elements is quite strong. In this regard IFN-γ seems to be significantly altered as well, which is another important marker with a distinct behavior. From [Ref2] “IFN-γ or IL-17 production by PBMCs -peripheral blood mononuclear cells- from any individual correlated independently of the identity of the pathogen stimulus”.
Results from [Ref0.2]:
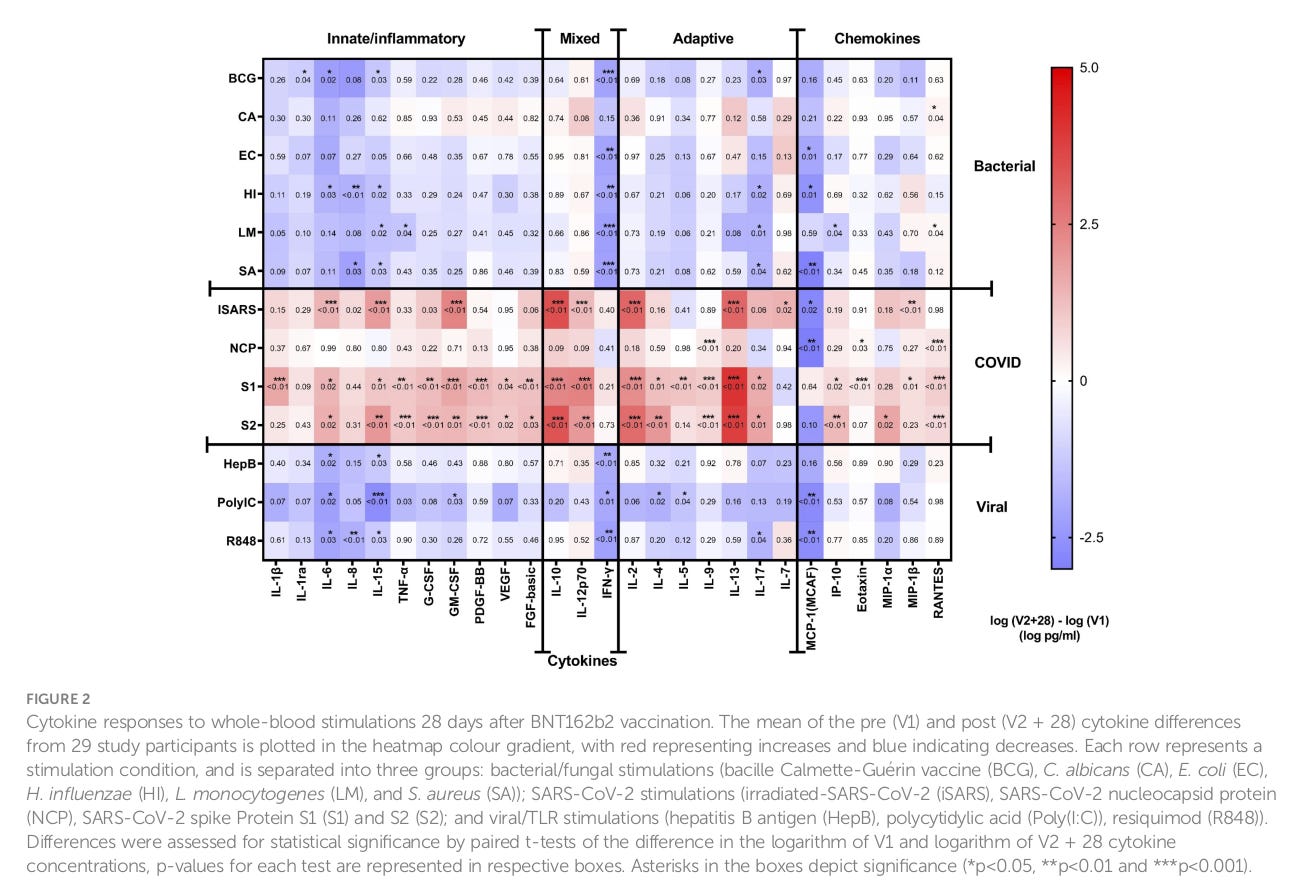

In fact if we consider the whole spectrum, and this is just me making a somewhat bold claim here, the shift towards strong responses to SARS-CoV-2 elements in vaccinated children is differentiating SARS-CoV-2 as a new “clade” distinct from virus or bacteria. I don't know… perhaps a specific immune response towards being transfected?
FINAL NOTE: Does the previous research demonstrate that Pfizer’s transfections causes VAIDS, i.e. Vaccine Acquired Immune Deficiency Syndrome?
[Link to my comment to Igor Chudov]
It does not and this is why:
If we pay close attention to what has been said before on my previous comment:
From [Ref1] [A systems immunology approach to investigate cytokine responses to viruses and bacteria and their association with disease] we highlighted that
“Patterns of human immune responses to viruses and bacteria and how this impacts risk of infections or onset/exacerbation of chronic respiratory diseases are poorly understood.”
“…we measured peripheral blood mononuclear cell responses (28 cytokines) to respiratory viruses and bacteria, Toll-like receptor ligands and phytohemagglutinin, in 307 children. Cytokine responses were highly variable with > 1000-fold differences between children.”
Thus, given that this phenomena is “poorly understood”, we can clearly acknowledge at the moment that any given conclusion would be a hypothesis. In order to clarify this issue farther, let’s take a look to a great immunology book, [Roitt's Essential Immunology] [Ref3] in which they state:
“…cytokines are involved in communication between cells of the immune system and help to alert the correct cell types that are appropriate for dealing with different classes (i.e., whether viral, bacterial, yeast, etc.) of infectious agents.”
“… In this way, detection of an infection (i.e., PAMPs *Pathogen-Associated Molecular Patterns*) by a particular class of PRR *Pattern Recognition Receptors* is translated into the most appropriate immune response through the production of particular patterns of cytokines and chemokines. These cytokine patterns then call into play the correct cell types and trigger maturation of these cells into even more specific effector cell subtypes.”
If we put together these two important notions, it is not the absolute amount of cytokines produced [“Cytokine responses were highly variable with > 1000-fold differences between children."], but the pattern they create, which gives [“the most appropriate immune response through the production of particular patterns of cytokines and chemokines”].
What we can clearly see on the study at hand [Ref0.2] [BNT162b2 COVID-19 vaccination in children alters cytokine responses to heterologous pathogens and Toll-like receptor agonists] is that there has been a shift in the priority given to different antigens, and as we mentioned before, given the changes in IFN-γ or IL-17, the immune system doesn’t seem to recognize antigens to the spike protein S as viral antigens. As I said before, this new cytokine pattern may be a specific respond to a transfection, which clearly is not viral or bacterial in origin.
A parallel investigation should be performed with the data originated by the same study [Ref0.2] to analyze if indeed there are changes in the cytokine patterns responsible for characterizing viral/bacterial/fungal… components before and after transfection, i.e. to compare the patterns, not the amounts of cytokines produced. Such patterns have already been shown in [Ref1]. As long as the pattern is constant, the absolute value of cytokine production does not necessarily mean immunodeficiency, but a priority shift of the immune system to the new threat of being transfected.
Of course, this is just my hypothesis, as I pointed out at the beginning, this phenomena is “poorly understood”. Nevertheless, another important conclusion that one can make from this data [Ref0.2] is that the immune system does not seem to reproduce an immune response equivalent to that of a natural infection from a coronavirus and therefore, the acquired immunization from this technique may be irrelevant or even counterproductive when presented with a natural infection, regardless of the presence or absence of neutralizing antibodies. The body will behave as if something different is happening, different from a viral infection that is. More studies are needed to make definitive conclusions in any case.
Now if we think of how gut bacteria like Clostridium difficile spread aggressively from person to person in a hospital setting...... or farming practices using human waste as fertilizer (which was hypothesized to be responsible for the wide prevalence of Covid in midwestern deer)......
The uncharacteristic IL17 response could also be due to the bacterial superantigen motifs that are encoded in the Spike.