


Supporting comment for the work of Denis Rancourt et.al. on Excess Mortality Analysis
In relation to the apparent delay shown in some countries

Hi Denis,
In relation to why some countries do not show a clear correlation with the vaccine rollout, presenting a peak before the campaign (winter of 2020-21) or after the campaign (winter of 2021-22, 2022-23) in the northern hemisphere, I think we have to consider the following, besides what you mentioned with regards to different age profiles:
From OECD.Stat methodological Note - "Some countries may refer to the date of death is registered (e.g. United Kingdom) rather than the actual date of death." "Some countries (e.g. the United States) may adjust their series to estimate the total number of deaths for the latest reporting periods. (Source) https://stats.oecd.org/wbos/fileview2.aspx?IDFile=97aacc20-eac4-4e44-8f59-9fb5b7e25090
[(NOTE) I included this comment on my substack in order to add some figures that would clarify the text. That may be useful to the reader who is not familiar with how the curves look like.]
Based on this and similar factors, there is a reason to believe that many countries adopted and shared a common strategy in order to register mortality data in a way that would avoid what they call "vaccine hesitancy". Maybe even as a national security threat or as part of the contracts with the pharmaceutical industry as well as the WHO, I cannot know. However, we can clearly see that all excess deaths are labeled as COVID in many countries, which is completely impossible due to the very distinct way in which excess deaths and deaths labeled as COVID are measured. It would never give the same result or even follow a similar trend, if done appropriately, without using estimates and forecasting based on the different predictors of mortality for different age cohorts, as well as subtracting normal deaths from seasonal influenza and pneumonia like illness, which is from where most deaths label as COVID are coming from. They are two completely different measurements with completely different dynamics, biases and error rates.

Thus, it may be the case that the excess deaths for the vaccination campaign were estimated, in advance, and the numbers were allocated appropriately to the sides of the campaign, either before it started or after it finished, while making sure that the same amount of deaths were registered as COVID deaths.
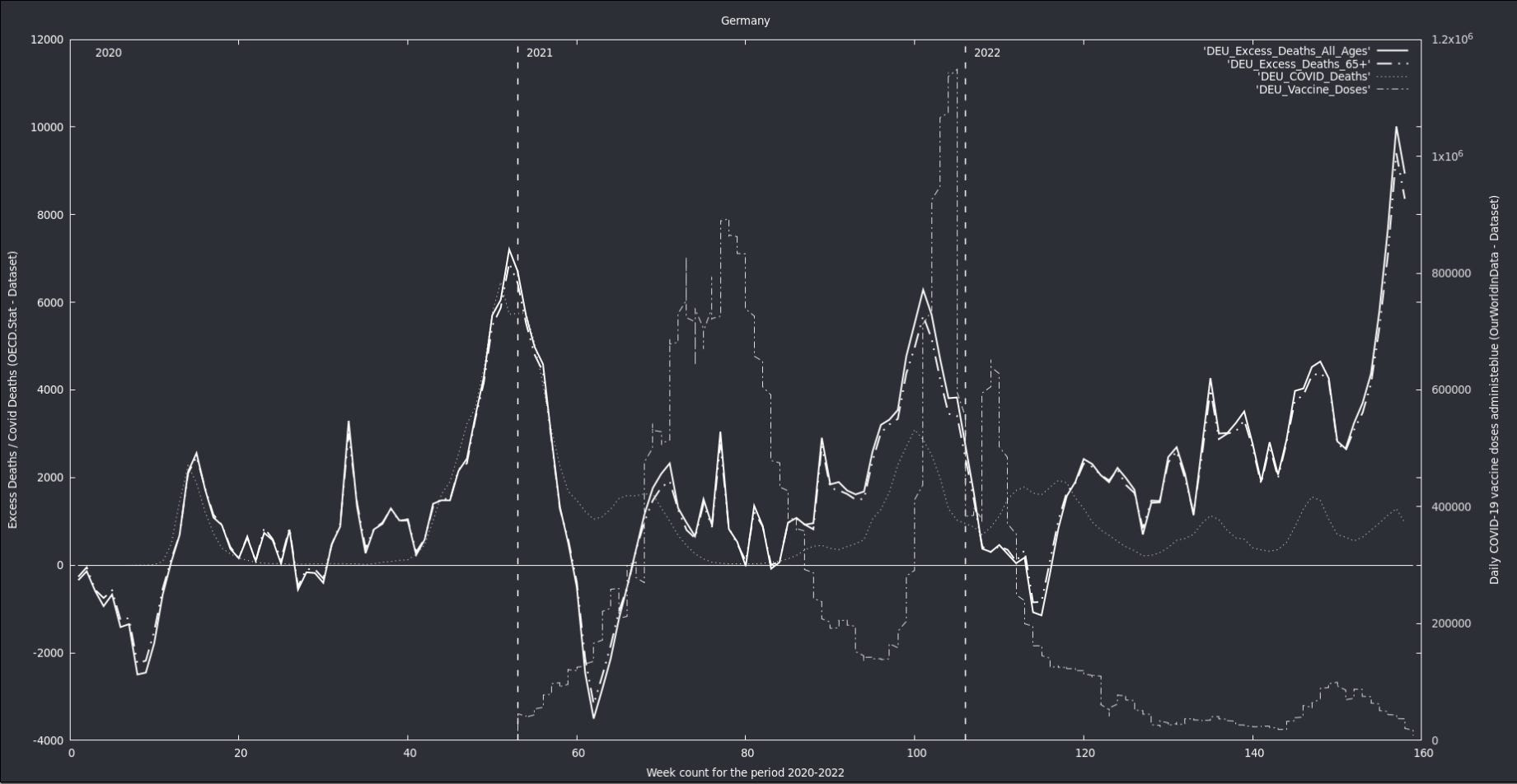
In some countries, like Germany for instance, I think they estimated excess deaths for 2021 a bit too low, making their 2020-21 winter peak relatively small. In this way, it seems plausible, that they ended up registering those deaths in the winter of 2022-23. By that time the COVID fearmongering was already gone in Germany so the last peak does not even correlate with deaths labeled as COVID, even though there was a limited number of vaccine doses given for that winter season. In any case, to my knowledge, nobody has adequately explained that last peak, which is quite considerable.
I don't think it is unreasonable to believe that a common strategy was shared among many countries under the guise of Emergency powers and the Public Health Emergency of International Concern (PHEIC) declaration. That may explain the odd features observed in some regions of the Globe and the delay between the vaccine rollout and the peak in excess deaths for the winters of 2021-22 and 2022-23.
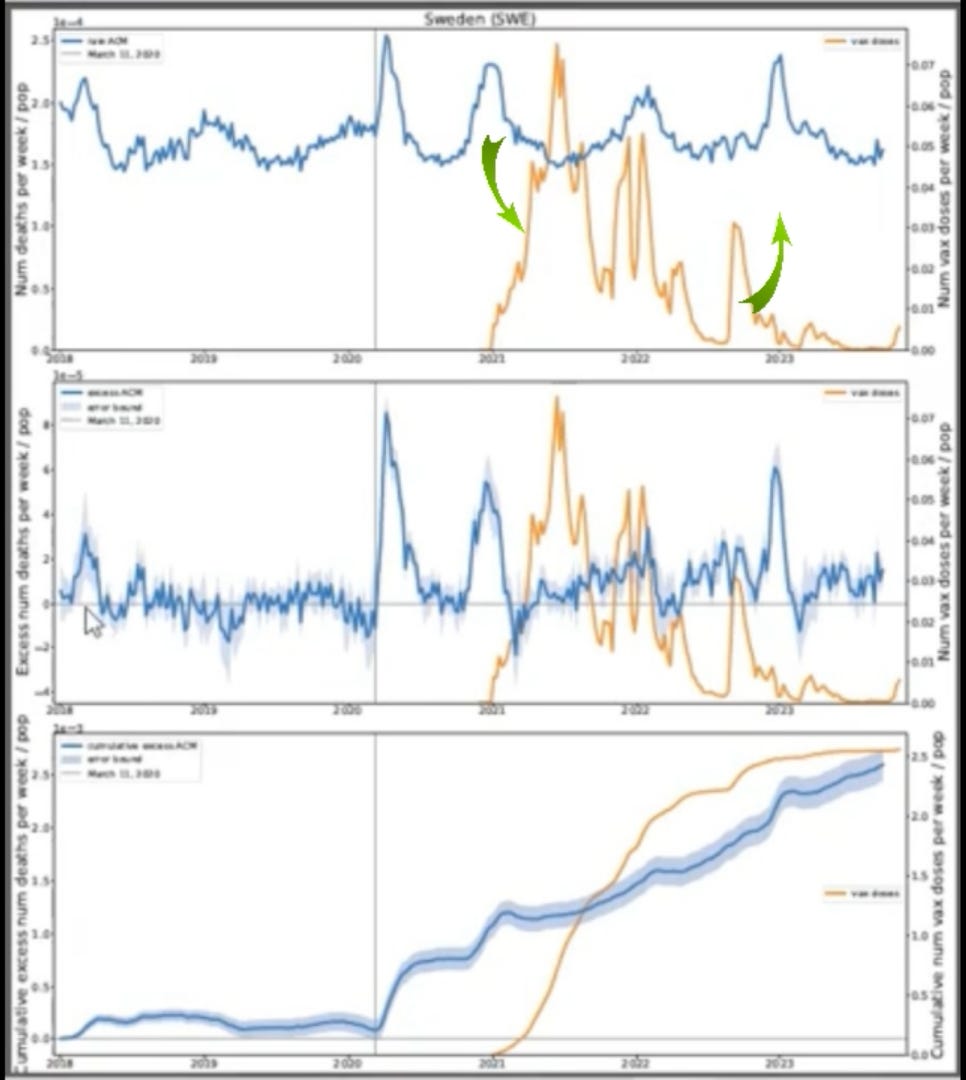
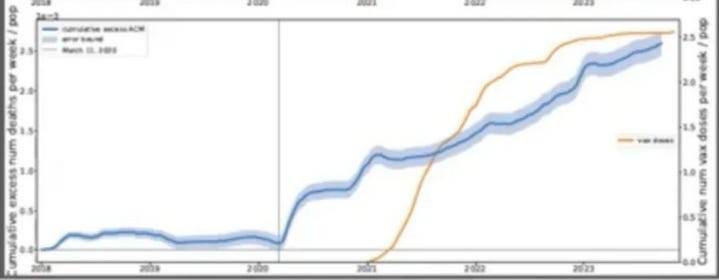
However, using your methodology and considering the general trend, we can clearly see an increase in excess deaths after the vaccine campaigns started, regardless of the apparent delays in the peaks of mortality.
(Link to my comment) https://denisrancourt.substack.com/p/my-response-to-tracy-beth-hoegs-criticisms/comment/48064317
(Comment to Tracy Beth Høeg, MD, PhD) https://www.illusionconsensus.com/p/a-critique-of-the-17-million-deaths/comment/48065123