

Reply to Igor's Newsletter: Ba.5 is a "Variant for Boosted People"
Reply to Igor's Newsletter: Ba.5 is a "Variant for Boosted People"
NOTE: I am just testing the system (this is my first substack). Making replies to other substacks will not be my focus.

Hi Igor,
I am sorry to say but... are we looking at the same charts?
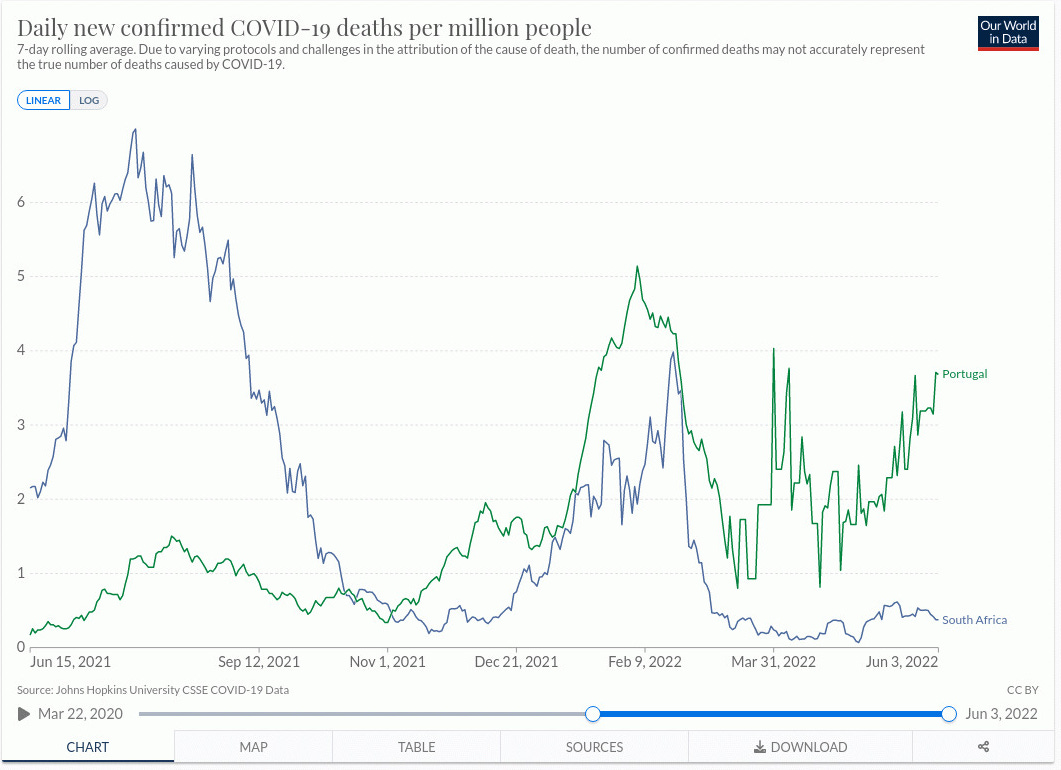
First of all, the cases chart is a complete fraud, it is completely correlated with how many tests have been done and I don't see any normalization in relation to that important value. Additionally, there are many other factors that make it impossible to compare the cases charts from one country to the next. So... let's focus exclusively on the deaths chart, where of course you have to consider still, that these are not deaths caused by SARS-CoV-2, these are people that have died with a positive test in some time frame defined by each country's Health Care System (hence… another serious difficulty in order to compare countries so easily with these charts).
But anyhow, that's the data that we have, I understand that. If we take a look at the charts, considering that Portugal is in Summer and South Africa is in Winter... the numbers are ridiculously low in both countries, 2-3 death per million on average. And... we are calling that a wave??? I would say… those numbers are noise and there is absolutely no signal from which you can even measure the noise level. And with that I mean… if you take those fake tests and the COVID-19 hysteria with a time machine to the year 1984 (where there is no SARS-CoV-2 at all, in principle) you would see that those numbers, are the noise level of your measurement. In fact, being the noise level correlated to other factors, like influenza, atypical pneumonia, respiratory diseases, seasonality, the media-propaganda itself and the fear-porn… (because you will increase the testing during those periods) you would even be able to replicate the waves with the noise level alone.
In any case… Are you honestly telling us that you see a difference in the death accounts between Portugal and South Africa because the numbers are still rising in Portugal? They will have to rise a lot, and that hasn’t happen yet. That’s my honest opinion.
Therefore I cannot agree with your conclusion:
*”It was no big deal for South Africa”
*”The same wave is deadly for the overboosted Portuguese and the deaths keep rising”
Reasons:
*It was no big deal in either place, still is no bid deal in Portugal now, and the dynamics in the epidemiological factors from winter to summer are very difficult to compare still. There are many other confounding factors that are relevant and there is not enough signal to sort them out.
*To see the effect of the booster, which is very relevant, I agree, we would have to select different cohorts within Portugal. It cannot be stated that Portugal is all boosted and South Africa is not boosted at all, and compare the two of them in relation to the booster factor. That is not robust or accurate and the conclusions that you may obtain by doing that can only be seen as early signals, if and only if in fact you have a SIGNAL. But there is no signal, I only see the noise values.
Conclusion:
I hope it helps and thanks a lot for your work, I’ve been following you for quite a while, great substack you have. My perspective may be wrong, but we all have to add something, this is a very complex subject. My background is in Biphysics and Complex Systems and I am on GETTR as Agus_Z. I am from the Iberian Peninsula so Portugal is just here next to me, and the same thing is happening in the whole Peninsula, nothing. Nothing significant anyway.
PS: In relation to the “cases” chart… I need the number of cases normalized to the number of tests performed. BY AGE GROUP if possible. Additionally, I would need to know which test kits (which manufacturers) has been used and the cycle threshold (Ct) values at which they have been working. Important is to know the number of tests performed by each laboratory and their actual capacity (how many tests they can accurately performed per day/week). That will give you an idea of how much contamination we are dealing with (the whole lab results should be thrown to the bin, if the lab ends up contaminated via mismanagement of positive controls, overcapacity, untrained staff…).
Of those tests used in the past, how many have been added to the list “Removal Lists of Tests That Should No Longer Be Used and/or Distributed for COVID-19: FAQs on Testing for SARS-CoV-2”? (1,2). I would also require a significant review on the “gene drop out” hypothesis in order to determine a positive test in relation to each SARS-CoV-2 variant and their prevalence (3).
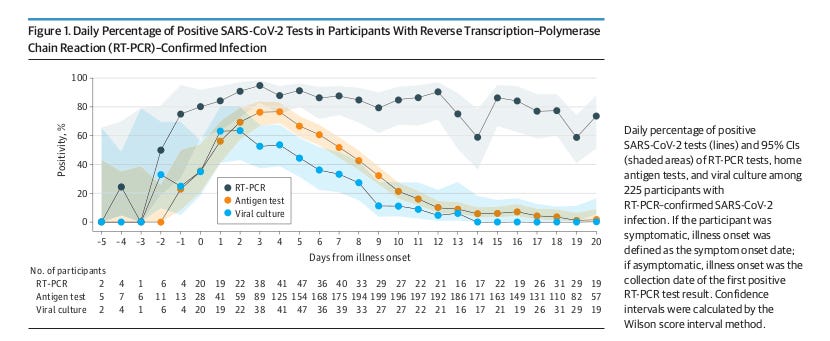
In fact, just to be accurate… I would discard as invalid any PCR test that is not accompanied by whole genome sequencing and has been clinically confirmed. I would do the same for any antigen/antibody test. They can only be considered as an early indication, even though, they seem to be more accurate, following the trend of a viral culture (4).
We have to remember though that “A CASE” MUST be someone that is clinically ill, not a healthy person. Finally, other molecular tests should be used in order to discard other possible causes, like influenza, Bacterial pneumonia, atypical pneumonia… for instance, which also helps to have a better understanding on how often co-infection is involved in a COVID-19 presentation.
And of course… you cannot forget, “cases” determined by whichever means,
MUST NEVER BE USED AS A POLITICAL WEAPON TO TERRORIZE THE POPULATION AND IMPLEMENT DRACONIAN MEASURES THAT ARE NOT EVEN RELATED TO ANYTHING BASED ON PUBLIC HEALTH, NOT EVEN IN THE SLIGHTEST!!!
(NOTE: I will collect all the relevant information regarding “testing” in a future substack, just to have it all organized in the same document. Otherwise, you have to jump from document to document and you can get crazy doing that.)
References:
(1) Certain COVID-19 Serology/Antibody Tests Should Not Be Used - Letter to Clinical Laboratory Staff and Health Care Providers
(2) In Vitro Diagnostics EUAs - Molecular Diagnostic Tests for SARS-CoV-2
(3) SARS-CoV-2 Viral Mutations: Impact on COVID-19 Tests
(4) Comparison of Home Antigen Testing With RT-PCR and Viral Culture During the Course of SARS-CoV-2 Infection

TESTING THE COMMENT SECTION
Hi Agus, I love your article and the healthy disagreement. I will respond later as I have to go shopping and stuff.
The deaths are 3.7 deaths per million PER DAY, this is equivalent to 1,221 deaths PER DAY in USA. Our latest in USA is 214 deaths per day. So it is not "nothing".
You do have a point about "cases", they are not counted properly so I did not dwell on them too much.